


Virtual Microscopy
|
|
||||
|
Virtual Microscopy |
||||
Case 1: Acute Hepatitis A
This 40 yo woman was seen by her primary care physician for 2 days of jaundice and abdominal discomfort following a 7 day period of flu-like symptoms including fever and arthralgias. She is taking no medications and denies prior blood transfusions, use of illicit drugs, and excessive ethanol ingestion. Laboratory evaluation revealed the following: ALT 883 IU/L, AST 409 IU/L, total bilirubin 10.7 mg/dl. Hepatitis B and C serologies were negative, but IgM anti-HAV was positive. Upon further questioning, she revealed that a friend was experiencing similar symptoms and they had dined at a new restaurant about a month ago.
Slides: [normal liver (including normal gallbladder)] [patient's liver]
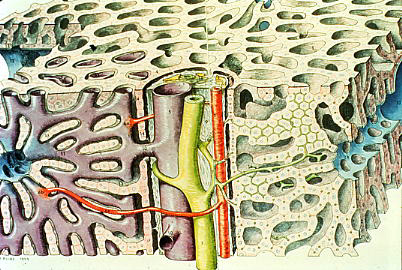
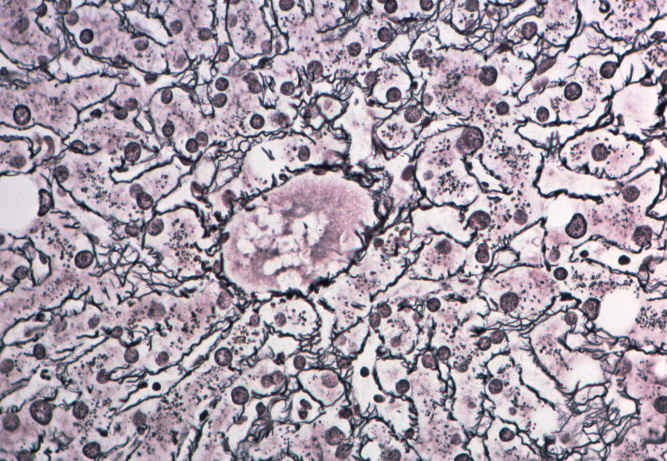
Gross images: [liver architecture] [normal liver (reticulin stain]
Case 2: Alcoholic Cirrhosis
This 45-year-old man was admitted to the hospital for evaluation of hematemesis (vomiting blood). He had a history of consuming one pint of whiskey per day for 20 years, but he had recently increased his intake. Two days prior to admission, he developed the abrupt onset of nausea and vomiting with bright red blood in the vomitus. Because of persistent hematemesis the patient came to the emergency room, where he was jaundiced and had ascites. Laboratory data included a hematocrit of 20, serum bilirubin of 4.5 mg/dl (direct 3.2), AST 100 IU/L, ALT 84 IU/L, serum albumin 2.7 gm/dl, and abnormal clotting function. The patient was stabilized, and underwent a liver biopsy was performed.
Slides: [patient's liver]
Case 3: Chronic Hepatitis due to Alpha-1 Anti-trypsin Deficiency
A 36-year-old woman with a family history of liver chronic liver disease and emphysema presents with elated liver function tests (bilirubin of 1.0 mg/dl, AST 147 IU/L, ALT 120 IU/L, serum albumin and clotting parameters normal). A liver biopsy was performed.
Slides: [normal liver] [alpha-1 anti-trypsin deficiency]
Case 4: Primary Biliary Cirrhosis
A 53-year-old woman presents with yellowing of her eyes and increasingly severe and irritating itching of her skin. On physical exam she is jaundiced, and has severe scratch marks covering her back except for the central most location. Her liver chemistries show a markedly elevated serum bilirubin and alkaline phosphatase but essentially normal transaminases (ALT and AST), albumin and clotting factors. An anti-mitochondrial (AMA) serum serology is strongly positive at a titer of 1:512. A liver biopsy is performed.
Slides: [normal liver] [primary biliary cirrhosis]
Case 5: Chronic Cholelithiasis with Cholecystitis
A 47-year-old obese, multiparous woman complained of abdominal pain, gas, and intolerance to fatty foods. Her physician performed an ultrasonic examination and found gallstones. The only treatment was advice to avoid foods that made her feel ill and to lose weight. Three years later, the patient returned with a one-day history of severe, cramping abdominal pain that radiated through to her back, nausea and vomiting. An ultrasound examination now showed dilated intrahepatic bile ducts. A cholecystectomy was performed and numerous gallstones were present.
Slides: [normal gallbladder] [chronic cholecystitis]
{kind=link}
{kind=link}