Virtual Microscopy > GI > GI Histology (SMALL AND LARGE INTESTINES AND PANCREAS)
Case 1: Ileal Crohn's Disease
A 27-year-old female presents with intermittent non-bloody diarrhea accompanied by moderate to severe cramping abdominal pain and a 15-lb weight loss. The pain is most severe in her right lower abdominal quadrant. Small bowel barium x-rays reveal a tight stricture in her terminal ileum and fistula between loops of small bowel. The strictured bowel is resected and a slide is presented for your study.
Slides: [normal ileum] [patient's ileum]
- Review the slide of normal small intestine. Be able to identify the following normal structures: mucosa, lamina propria including mucosal associated lymphoid tissue (MALT) or Peyer's patches, muscularis mucosae, submucosa, muscularis propria, and adventitia.
- Scarring and inflammation with discrete lymphoid aggregates are seen in what areas of the patient's resected bowel?
- In addition to scarring and discrete lymphoid aggregates, do you see any cells types that are not normally present in the small intestinal mucosa, or bowel wall?
- How might these changes have resulted in diarrhea and abdominal pain?
Case 2: Acute appendicitis
A 12-year-old boy presents with vomiting and abdominal pain. His white blood count is 2 times normal and he has a fever. His abdominal examination reveals right lower quadrant pain. He is taken to the OR for an appendectomy.
Slides: [normal appendix] [patient's appendix]
- Review the section of normal appendix. Be able to identify the following normal structures: mucosa, lamina propria including mucosal associated lymphoid tissue (MALT) or Peyer's patches, muscularis mucosae, submucosa, muscularis propria, and adventitia.
- What cells are present in the patient's resected appendix that are not seen in the normal appendix?
- Are any normal cell types missing?
- How might the pathologic process have produced the patient's signs and symptoms?
Case 3: Colonic Adenoma
A 52-year-old man presents for a screening colonoscopy as part of a standard colonic cancer prevention program. A polyp was identified and removed endoscopically and is provided for your study.
Slides: [normal colon] [patient's polyp]
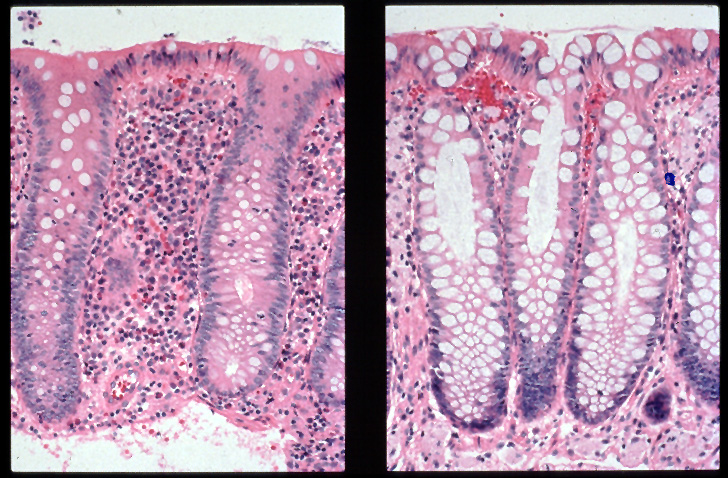
Other images: [normal right versus left colon]
- Review the section of normal colon. Be able to identify the following normal structures: mucosa including the epithelial cells, lamina propria, muscularis mucosae, submucosa, muscularis propria, and adventitia.
- What are the differences between the epithelial cells on the resected polyp and those of normal colonic epithelium? Compare the cytoplasm and the nuclei and the architecture or growth pattern of the epithelial cells.
- Why were these polyps removed?
Case 4: Colonic Adenocarcinoma
A 65-year-old man presents with increasing constipation and blood in his stool. He has never undergone colorectal cancer screening tests. A colonoscopy with biopsy was performed followed by surgical resection of an obstructing colonic mass directly adjacent to a residual mucosal polyp. A section is provided for your study.
Slides: [patient's colon]
- What structures of the normal colonic wall are being replaced by the tumor? How deeply does the tumor penetrate?
- What kind of epithelium is the tumor composed of (glandular or squamous)?
- Are there differences in the tumor cells relative to the normal colonic epithelium or to the adjacent polyp?
- How might this cancer have been prevented?
Case 5: Chronic Pancreatitis
A 48-year-old male chronic alcoholic developed persistent, cramping, periumbilical abdominal pain. He had lost 25 lb of weight despite a good appetite and eating large amounts of food. He had also noted the onset of intermittent diarrhea and a change in the character of his stools, which he described as malodorous and "greasy" looking. His serum glucose was elevated. Because his pain became severe, intractable, unresponsive to narcotics and debilitating, a pancreatectomy was performed. A slide of this and of normal pancreas are submitted for your study.
Slides: [patient's pancreas] [normal pancreas]
- Review the slide of normal pancreas. Be able to identify the following normal structures: acinar cells, ducts, and islets.
- What normal pancreatic cells and structures are missing in the patient's resection material? What new cell types are present?
- How might the pathologic process affect the normal functions of the pancreas?
- Why might the histologic changes have resulted in the patient's change in bowel habits?
- Can you theorize as to why his serum glucose was elevated?



{kind=link}